
Toe walking treatment and management
The management of toe walking is controversial — the natural history is poorly defined, and only limited data are available regarding direct comparisons of different treatment modalities.
Therefore, the physician’s first decision point is whether the toe-walking gait should be treated at all or whether simple observation should be recommended.

Cascade DAFO
By Ryan Krochak MD, Chief Editor: Vinod K Panchbhavi MD FACS, Medscape Updated February 19, 2019
| Overview |
| Background |
Toe walking is a gait abnormality characterized by an absence of normal heel-to-floor contact (heel strike) by both feet during gait. It is defined as the inability to make heel contact with the floor during the initial stance phase of the gait cycle and the absence of full foot contact with the ground during the remainder of the gait cycle. The forefoot engages in the majority of floor contact throughout the gait cycle.
Toe walking has multiple etiologies, ranging from idiosyncratic habit to profound neuromuscular disease. The most commonly observed type of toe walking is idiopathic toe walking (ITW), which is a diagnosis of exclusion. Toe walking that results from a definable cause (most often neurologic or muscular disease) can be broadly labeled non-idiopathic toe walking (non-ITW). Identification of non-ITW is critical for determining appropriate treatment and understanding recurrence rates.
Although toe walking is commonly seen during development in children who are first learning to walk, a consistent heel-toe pattern of gait usually develops by approximately age 22 months.[1,2] If toe walking persists beyond age 2 years, further evaluation is warranted.[3]
Treatment depends on the patient’s age, the severity of the gait abnormality, and the underlying diagnosis. Specific treatment options range from simple observation to surgical lengthening of muscles or tendons in the lower extremity. Achilles tendon tenotomy is the commonly used procedure for the treatment of toe walking and is one of the oldest procedures in orthopedics.[4]
| Anatomy |
The triceps surae muscle-tendon complex is the confluence of the gastrocnemius and soleus muscles and the Achilles tendon or heel cord, the largest tendon in the human body.
The gastrocnemius muscle originates from the posterior medial and lateral femoral condyles and inserts onto the calcaneus through the Achilles tendon. It crosses both the knee and the ankle joints and acts as a major plantarflexor of the ankle and a minor flexor of the knee. It typically has more fast-twitch type II muscle fibers, which are responsible for short, powerful bursts of activity such as running and jumping.
The soleus muscle lies deep (anterior) to the gastrocnemius and originates from the posterior surfaces of the proximal tibia and fibula and inserts into the calcaneus by way of the conjoined Achilles tendon. It crosses only the ankle joint and functions to plantarflex the ankle. The soleus muscle is made up of primarily slow-twitch type I muscle fibers and is responsible primarily for postural control.
The Achilles tendon measures approximately 4-8 cm from the point where the gastrocnemius and soleus muscles join to its insertion on the calcaneus. As the fibers of the tendon traverse this distance, they rotate approximately 90º in the axial plane. The fibers from the more superficial gastrocnemius muscle insert on the posterolateral aspect of the calcaneus, and the fibers from the deeper soleus muscle insert on the posteromedial aspect of the calcaneus.[5] Understanding this rotation of the fibers helps in planning the percutaneous lengthening procedure (see Surgical Therapy).
It is possible to separate the contributions of the gastrocnemius and soleus muscles to an equinus ankle contracture via the Silfverskiöld test. According to this test, increased ankle dorsiflexion with the knee in flexion compared with the knee in extension indicates gastrocnemius tightness. This occurs because the gastrocnemius relaxes with knee flexion as the muscle spans the knee joint, whereas the soleus does not. If there is no difference in dorsiflexion with knee flexion, an Achilles tendon contracture is present. The test assists in deciding the surgical approach to lengthening of a patient’s heel cord.
| Pathophysiology |
Although the exact pathophysiology of ITW remains unknown, it is postulated that mild defects in sensory processing exist in affected children and that this gait may result from a vestibular disorder or abnormal sensitivity to touch.[6] However, there is limited research exploring these relations.
ITW likely has a genetic component, in that a positive family history has been reported in many case series.[7] In the initial description of the condition, Hall et al noted that all their patients had congenital shortness of the Achilles tendon, which led to ankle equinus and toe walking.[8] However, subsequent studies found that not all patients with ITW exhibit a congenitally short Achilles tendon as a mechanical explanation for the gait difference and that some patients toe-walk despite a volitional ability to walk flatfooted (“dynamic” or “habitual” toe walkers).[7]
Causes of non-ITW may be broadly separated into neurologic and muscular etiologies, classic examples of which are cerebral palsy (CP) and Duchenne muscular dystrophy (DMD), respectively.
In patients with CP, the pathophysiology of toe walking is clearer and is thought to be a product of two basic mechanisms resulting from lower-extremity muscle spasticity, as follows:[9]
- First, spasticity of the foot and ankle muscles can lead to progressive ankle equinus contracture as spastic muscles grow at a slower rate than muscles that are not spastic
- Second, spasticity and flexion of the more proximal hip and knee joints can result in apparent toe walking as the patient attempts to maintain balance when upright; if the hip and knee are flexed in stance and the ankle is held at a right angle relative to the tibia (plantigrade), the patient bears weight on the toes and forefoot, even though the ankle itself is not in equinus
In DMD, lower-extremity muscles progressively weaken as they degenerate and are replaced by fibrous tissue. Toe walking results from the relatively greater weakening of the dorsiflexors of the foot as compared with the plantarflexors. Toe walking also develops to compensate for the weakening quadriceps muscle. As the quadriceps weakens, active knee extension is lost, and the knee preferentially buckles into flexion with each step. By walking on the forefoot, the patient generates a knee-extension moment that aids in providing knee stability.[10]
| Etiology |
The etiology of toe walking is broadly separated into two categories, ITW causes and non-ITW causes. Non-ITW causes include both central and peripheral neurologic disorders (eg, tethered cord, diastematomyelia, spina bifida, and cerebral palsy), muscular disorders (eg, congenital muscular dystrophy), and anatomic disorders (eg, limb-length discrepancy).[3] Some rarer causes of toe walking have also been reported in the literature, such as acute toe walking secondary to viral myositis in a previously healthy 4-year-old child.[11]
ITW is the most common form of toe walking (with the term idiopathic understood to mean that no identifiable pathologic process exists to explain the perceived gait abnormality).
ITW, first described by Hall in 1967 as “habitual toe walking” and “congenital short Achilles tendon,” is a diagnosis of exclusion.[8] It is best defined as bilateral toe walking with or without Achilles tendon contracture in a child older than age 2 years in the absence of other identifiable causes. (See Physical Medicine and Rehabilitation for Spasticity, Spinal Cord Trauma and Related Diseases, Muscular Dystrophy, and Congenital Myopathies).
| Epidemiology |
The true prevalence of ITW is unknown because not all children with this condition present to a physician.
In several small studies, ITW was estimated to occur in 7-24% of the childhood population.[12] A large Dutch cross-sectional study from 2011 found a prevalence of 12% in the general population.[12] A large Swedish study from 2012 found the prevalence of ITW to be 4.9% in children aged 5 years 6 months.[13] A comprehensive literature review published by Ruzbarsky et al in 2016 found the prevalence at 5.5 years to be 2% in normally developing children and 41% in children with a neuropsychiatric diagnosis or developmental delay.[14]
ITW is observed more frequently in patients with autism, developmental delay, and language disorders.[7] A 2011 study determined the incidence of toe walking in children with autistic spectrum disorder to be 20.1%, whereas historical reports estimated it to be as high as 63%.[15] Conversely, children with ITW display an increased prevalence for other pediatric neuropsychiatric disorders, such as attention-deficit/hyperactivity disorder, tics, Tourette syndrome, and obsessive-compulsive disorder.[16]
A 2016 article by Baber et al reviewed the birth characteristics of children with ITW or toe walking due to medical reasons.[17] They evaluated 95 children diagnosed with ITW (mean age, 5.8 ± 2.9 years). These children were found to have higher rates of prematurity, higher rates of admission to a special care nursery or neonatal intensive care unit, and lower birth weights than the normative population. Children with a medical reason for toe walking also had greater rates of prematurity than the normative population and more instrumented births than children with ITW.
Baber et al found no association between assisted-birth intervention and the ITW cohort in comparison with the normative population or the medical-cause cohort.[17] ITW gait was associated with higher rates of complications during and after delivery. Such complications have previously been cited as risk factors for neurologic insult affecting motor development.
The most common cause of non-ITW is CP, which affects 1-7 in 1000 children. Reports vary greatly regarding the incidence of toe walking in this population, largely because of the wide spectrum of disease severity. Generally, fewer than 50% of these patients walk on their toes.[18]
DMD is the most common primary muscle-disease etiology of non-ITW. It has an incidence of 1 case per 3500 live male births and is the most common degenerative muscle disease of childhood.[19] The typical child with DMD initially walks with a heel-to-toe pattern but progresses to a consistent toe-walking pattern as a product of Achilles tendon contracture and a compensation for knee extensors.
| Prognosis |
The natural history of ITW remains poorly defined. Most studies offering long-term follow-up for untreated patients concurrently report treatment of their cohorts. Opinion on the adult consequences of a persistent toe-walking pattern are generally divided into two schools of thought.
The first school of thought holds that regardless of the initial status of the heel cord and ankle range of motion (ROM), children with persistent toe walking eventually develop a fixed ankle contracture and ankle equinus in adulthood, which lead to hindfoot valgus and myriad potential foot disorders.[20, 21, 22, 23, 24] This argument supports aggressive intervention for ITW in early childhood.
The second school of thought holds that ITW can have a benign natural history, with the majority of patients manifesting no particular functional limitations or pathologic sequelae in adulthood, despite variable objective improvement in overall ankle ROM or gait.[25] This argument supports an observational approach to management of this gait abnormality.
The long-term results of treatment for ITW are unclear, mostly because of an unclear comparative natural history but also because of a tendency of the studies to mix a variety of management methods.
Reported outcomes of treatment of ITW with stretching casts have been variable. In a long-term study of 14 children with ITW treated with a stretching regimen with or without casting, only three children required additional treatment for persistent toe walking after several years.[26] However, in a larger series, no difference in outcome was seen between patients treated with observation and those treated with serial casting: 50% of both groups had improvements in gait.[25] Other studies showed similar variability, with one finding 66% of patients to have improved ankle dorsiflexion and gait after casting.[25, 27, 28]
Overall, casting management seems to be most successful in patients with an initial ankle dorsiflexion of greater than 0º. In addition, recurrence of toe walking is unlikely in patients who have spontaneously discontinued toe walking or who remain down on their heels for more than 1 year after casting treatment.[3]
Surgical management of ITW, through either complete Achilles lengthening or isolated gastrocnemius lengthening, appears to be effective in the appropriate clinical setting.[29] In one study, 72% of surgically treated patients reported a normal or improved gait at follow-up.[25] In another, all surgically treated patients showed improvement in ankle dorsiflexion, and the reported parental satisfaction rate was 67%.[28] Long-term outcome studies suggest that surgical management is more effective than nonsurgical management. However, direct comparison is difficult, owing to the variability of patient age and disease severity in these studies.[25]
The natural history for patients with non-ITW from spasticity or paralytic muscle disease is generally thought to be one of persisting ambulatory instability, given the poor balance mechanics afforded by the overriding disease process coupled with the poor base of support from the foot position. Intervention is more often recommended for this patient population for the purpose of improving gait stability. However, interventions for toe walking are also less predictable in this population, and patients often require long-term follow-up to monitor for recurrence.[30]
In patients with CP, treatment of ambulatory individuals without a fixed ankle contracture by means of full-time bracing (ankle-foot orthoses [AFOs]) has been shown to have a positive effect on ankle ROM and power at pushoff.[31] Among CP patients who have a rigid deformity, children younger than 7 years at the time of surgery have been shown to be at greater risk for recurrence. Hemiplegic patients have also been found to have higher recurrence rates than diplegic patients.[32]
However, surgical lengthening can have lasting results. In one long-term study, surgical lengthening in CP patients with a fixed equinus contracture resulted in a significant gain in average dorsiflexion, from –25° preoperatively to 8° postoperatively, and this correction was maintained by stretching and AFOs in 80% of patients 7 years after the index procedure.[33]
Randomized controlled studies have not shown botulinum toxin alone to offer better long-term outcomes than casting alone for dynamic equinus in children with CP or ITW.[34, 35] Furthermore, combining botulinum toxin injections with casting has not been shown to yield improved results as compared with casting alone for either toe-walking CP patients or patients with ITW.[34, 35]
| Clinical Presentation |
| History |
A child with idiopathic toe walking (ITW) typically presents as a toddler, without other significant medical history and with a normal developmental profile, especially a normal age for the commencement of walking (before 18 months). The parents report that the child walks and runs on the toes of both lower extremities symmetrically, particularly when he or she is unaware of being observed. However, the child often can walk flatfooted if prompted.
The presentation of toe walking in a patient with a discrete central or peripheral nervous system etiology (non-ITW) differs from that of a patient with ITW. In a patient with cerebral palsy (CP), there is often a history of prematurity and of global developmental delay, especially a delayed age at which the child began walking. There may also be a history of a significant head injury or vascular event before age 2 years.
Other features upon presentation that may suggest non-ITW include the following:
- History of spinal cord injury
- Progressive loss of lower-extremity function
- Asymmetric progressive lower-extremity deformity
Specific spinal cord lesions that can result in asymmetric toe walking include spinal cord tumor and split-cord malformation/diastematomyelia.
A patient with toe walking secondary to a degenerative muscle disease usually presents later, in the age range of 3-5 years, often after the primary diagnosis has been established. The developmental history or past medical history in this patient population is typically normal.
The differences in presentation between the various patient groups can be subtle and subject to overlap. Therefore, it is imperative that the examiner routinely review the child’s perinatal history, developmental history, and past medical history, as well as obtain a detailed history of present illness, so as to minimize the likelihood of missing a diagnosis with significant long-term medical implications for the patient.
| Physical Examination |
The examiner’s responsibility in evaluating a patient with toe walking is to rule out all defined etiologies before settling on a diagnosis of ITW.
The examination should begin with an overall assessment of patient appearance and gait. Gait can be observed as the patient moves about the room or walks down a hallway. (See the images below.) A focused examination of the spine and lower extremities is then required. The child’s lower extremities and spine should be inspected for cutaneous abnormalities, leg-length discrepancy, asymmetric or abnormal muscle development, pelvic asymmetry, and fixed-foot deformities.

Idiopathic toe walking in 10-year-old boy: rear and side views. Medscape
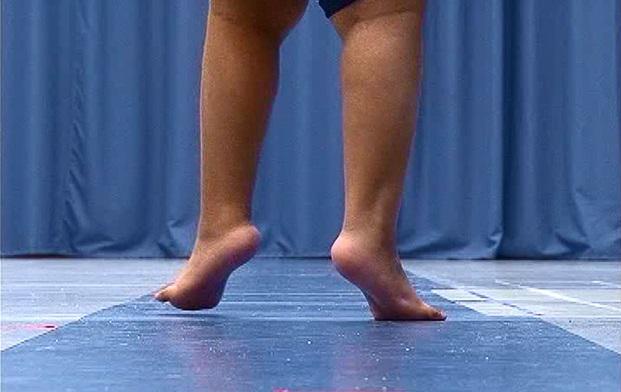
Idiopathic toe walking in 10-year-old boy: closeup view. Medscape
Although a thorough neurologic examination is challenging in this age group, muscle strength can be gauged by the ability of the child to rise independently from the floor and to climb the examination table. Reflexes, muscle tone, and withdrawal to stimuli are easier data points to acquire.
Assessment of range of motion (ROM) of the knee, hip, and ankle joints completes the examination. Ankle ROM should be assessed with the knee both flexed and extended (Silfverskiöld test). In addition, ankle dorsiflexion should be examined with the heel in neutral position; hindfoot valgus gives the false appearance of acceptable dorsiflexion.
For the patient with ITW, the examination is normal except for the symmetric presence of bilateral toe walking and a variable degree of heel-cord tightness. An asymmetric toe-walking profile essentially excludes the diagnosis of ITW and prompts further investigation.
Pomarino et al evaluated ITW pattern in 836 children, employing specific tests that had not previously been used by any other researchers.[36] The children were analyzed over a period of 4 years. Questions regarding family history were recorded. Tests included ankle dorsiflexion, lumbar lordosis angle, clinical spin test, walking after spin test, and heel walking test, which revealed that in all cases, children with a positive family predisposition were significantly more affected than children with a negative family predisposition. This study was aimed at developing new tools for improved diagnosis of ITW.
In a patient with a central nervous system disorder (eg, CP), muscle spasticity is apparent at the time of the initial evaluation, and deep tendon reflexes are hyperactive. Gait evaluation suggests overall difficulty with coordination and balance, as well as different degrees of upper-extremity flexion posturing, depending on the extent of involvement. The anatomic distribution of the spasticity should be noted; this is correlated with the extent of the lesion of the motor cortex. In addition, the examiner should determine if the toe walking is secondary to Achilles tendon contracture or if it is a compensation for spastic knee and hip flexion.
In a patient with muscular dystrophy, the classic findings are lumbar lordosis, calf hypertrophy, and a positive Gower sign (ie, the need to prop oneself up on the thighs with the arms in order to rise from a seated position on the floor). Strength examination suggests greater weakness of proximal hip and shoulder muscles.
| Workup |
| Laboratory Studies |
Measurement of serum creatine phosphokinase (CPK) may be useful to confirm muscle disease as the suspected etiology of toe walking. CPK levels are markedly elevated in Duchenne muscular dystrophy (DMD).
| Imaging Studies |
Although no formal imaging studies are required for a routine evaluation of toe walking, the studies discussed below may be used to gain more insight into the etiology of this condition.
| Plain radiography |
Standing anteroposterior (AP), lateral, and oblique radiographs of the feet are obtained to provide a more objective assessment of ankle equinus and rule out a possible bony foot or ankle abnormality as a cause for the toe walking.
In a patient with muscle spasticity that is not secondary to cerebral palsy (CP) or in a patient with isolated lower-extremity weakness, posteroanterior (PA) and lateral radiographs of the thoracolumbar spine are indicated to rule out bony abnormalities that may suggest a spinal-cord abnormality. Large posterior-element defects and a widened distance between pedicles might indicate an intraspinal anomaly
| Magnetic resonance imaging |
If the findings from plain radiography are positive or if clinical suspicion of a focal neurologic abnormality is high, magnetic resonance imaging (MRI) of the spinal cord, the brain, or both should be obtained as a definitive screen for the possibility of a focal pathologic process in the central nervous system. MRI of the spine in younger patients invariably necessitates sedation services to allow a good-resolution study.
| Other Tests |
Additional diagnostic tests are not routinely required for the evaluation of toe walking; their use is guided by the specific clinical scenario. Some controversies exist regarding the widespread use of electromyography (EMG) and gait analysis in diagnosis. However, both evaluations may be helpful in select patients.
| Electromyography |
EMG may be performed if the family history or clinical symptoms are suggestive of hereditary sensorimotor neuropathies. Dynamic EMG data can also be obtained from surface or intramuscular electrodes so that muscle activity can be correlated with the phases of the gait cycle. It has been shown that children with idiopathic toe walking (ITW) and CP have premature activation of the gastrocnemius muscles during the swing phase of gait as compared with normal children, in whom activation is seen only in the stance phase.[37]
EMG can also differentiate ITW from CP. Children with CP demonstrate coactivation of the gastrocnemius-soleus complex along with the quadriceps muscles during stance, whereas children with ITW do not.[38, 39]
| Gait analysis |
Although formal computerized motion analysis facilities are not universally available, several studies have shown that such analysis can help distinguish ITW from mild CP when the distinction is not readily apparent on physical examination.[40, 41]
O’Sullivan et al carried out a gait laboratory review of 102 patients who presented with a presumptive diagnosis of ITW.[42] Through analysis, they found that 81 (79.4%) of the cases had data that agreed with this presumptive diagnosis, whereas 21 (20.6%) were not typical of this diagnosis. There were significant differences between the groups with respect to Babinski response, fast stretch of the gastrocnemius, knee flexion at initial contact, and asymmetry at the ankles during gait.
This study highlighted the useful applications of this noninvasive means of diagnosis, which can help guide appropriate treatment while avoiding inappropriate procedures.[42] Gait analysis can also be particularly helpful in a patient whose toe walking has a spastic etiology, in that it helps separate the multiple joint and muscle contributors to the observed gait. For example, gait analysis can help determine whether toe walking is caused by ankle plantarflexor spasticity alone or by a combination of muscle spasticity at the knee and hip.
| Toe-walking tool |
The toe-walking tool is a reliable and validated 28-item questionnaire designed to aid practitioners in identifying underlying medical conditions that lead to a toe-walking gait. It can be the primary focus of an algorithmic approach to the evaluation of a patient with toe walking.[43]
| Auditory feedback |
An auditory feedback system to assist in gait rehabilitation of CP patients with dynamic toe walking has been developed. Based on plantar pressure monitors embedded in shoes, this system can monitor toe-walking strides in real time and produce an auditory signal to alert patients when toe walking has been detected. Although this system was designed to identify toe-walking strides in children with CP, its use may also be expanded in the future to provide a behavior-modifying feedback system for children with ITW.[44]
| Procedures |
Muscle biopsy is a surgical procedure previously used to confirm muscle disease as the suspected etiology of toe walking.[24] Currently, muscle biopsy is rarely used in this setting, because genetic tests are increasingly capable of offering similar information without the associated procedural morbidity.
| Treatment & Management |
| Approach Considerations |
The management of toe walking is controversial; the natural history is poorly defined, and only limited data are available regarding direct comparisons of different treatment modalities. Therefore, the physician’s first decision point is whether the toe-walking gait should be treated at all or whether simple observation should be recommended.
Observation is appropriate for a toddler with idiopathic toe walking (ITW) who has recently begun to walk and is without fixed contractures. In many children, this condition is only a temporary habit, and a normal heel-toe gait eventually develops.[1, 2]
The patient should be monitored at 6- to 12-month intervals. If progressive heel-cord contractures are detected or if the pattern does not resolve spontaneously by age 3 years, treatment can be considered. Treatment is not necessarily required for a child with ITW who is without discomfort or functional limitations and who tolerates the cosmetic component of the toe-walking posture.
Treatment is usually offered to a patient with an underlying neurologic or muscle abnormality, on the grounds that such patients are thought to benefit in ambulation from plantigrade positioning of the foot with gait.
If treatment is offered, nonoperative management (see Medical Therapy) is the therapeutic mainstay and is always considered before operative management (see Surgical Therapy). If nonoperative modalities are not successful and surgery is chosen, options range from simple heel-cord tenotomy to multiple-muscle lengthening within the lower extremity. The optimal approach varies, depending on the underlying etiology of the toe walking.
| Medical Therapy |
Nonoperative treatment of toe walking includes stretching, casting, orthotics, and chemodenervation with botulinum toxin. The success of such treatment depends on the age of the patient, the severity of the equinus deformity, and the underlying etiology.
Stretching exercises are often the first treatment attempted for toe walking because stretching is the least invasive therapeutic measure. It is recognized that stretching and physical therapy offer a limited chance of success in treating ITW; accordingly, they are more often used in an attempt to maintain range of motion (ROM) gained by means of other methods.[7]
Stretching exercises must leverage the patient’s body weight; the lower-extremity muscles are too powerful to allow effective passive stretching by parents or therapists. In one technique, the child is stood with the forefoot elevated on a small block so that the heel may drop downward. The parents steady the child and add gentle pressure to the stretching process. In a second technique, the patient leans forward against a counter, with feet together and pointed straight forward, knees straight, and hips extended. Progressive stretch is accomplished by increasing the distance from the counter.
Williams et al studied the effect of applying whole-body vibration on heel strike, spatial and temporal gait parameters, and ankle ROM in children with ITW.[45] Pre-intervention ankle ROM was compared with ROM immediately after and 20 minutes after intervention. Increases in heel contact and ankle ROM were observed immediately after intervention but were not sustained 20 minutes later. The gait improvement from whole-body vibration could be due to a rapid increase in ankle ROM or to a neuromodulation response. This potential treatment modality presents a nonrestrictive form of treatment, but its effects may not be lasting.
Serial casting is another nonoperative technique for stretching the Achilles tendon.[27] The child is placed in a below-the-knee plaster or fiberglass cast while the knee is flexed and the foot is dorsiflexed. This is most easily done with the child prone and with an assistant pushing gently downward on the forefoot. Once the cast has set, the gastrocnemius component stretches further as the knee extends. These casts are changed weekly or biweekly to progressively increase the range of dorsiflexion. Between cast changes, the child can walk with the use of cast shoes.
A custom orthotic, such as an articulated molded ankle-foot orthosis (AFO; see the image below), is another option for nonoperative treatment. This appliance is cosmetically acceptable, fits in a regular shoe, allows nearly normal ambulation, and prevents plantarflexion while allowing full dorsiflexion with every step. An AFO in a growing child can be expected to fit for 12-18 months before requiring replacement.
For toe walking due to muscle spasticity, stretching alone is ineffective.[31] Serial casting can be used to lengthen the Achilles tendon, but the contracture recurs rapidly unless the patient is maintained in an AFO. An articulated molded AFO, if used consistently, is an effective appliance for preventing the progression of spastic equinus that occurs with growth. If a patient with spasticity continues to toe-walk when AFOs are discontinued after the patient reaches skeletal maturity, operative lengthening may then be considered so that the orthosis can be discontinued. After skeletal maturity, equinus in a patient who is spastic is less likely to recur.[9]
Chemodenervation of the gastrocnemius-soleus complex muscles with botulinum toxin is yet another method of nonoperative treatment. Botulinum toxin causes temporary (~3 months) selective muscle paralysis by blocking acetylcholine release at the neuromuscular junction. It was first introduced in the early 1990s as an injection into the gastrocnemius muscle in an attempt to decrease tone in patients with cerebral palsy (CP).[46] Subsequently, its suggested indications expanded to ITW, but most studies have found it to have little efficacy in this application.[34]
A 2014 review of the literature by van Kuijk et al found preliminary evidence for beneficial effects of serial casting and surgery on passive ankle dorsiflexion, as well as on walking kinetics and kinematics, though normalization does not seem to occur.[47] In this article, botulinum toxin type A was not found to improve the results of casting. Only after surgery were sustainable effects lasting longer than 1 year reported. Effectiveness with respect to functional activities and social participation has yet to be demonstrated.
For toe walking associated with paralytic muscle disease, the use of regular stretching and orthoses together should be considered while the child remains ambulatory. Both modalities of nonoperative treatment are preferable to operative lengthening, which weakens the muscle and interferes with ambulation. Prolonged use of serial casts also weakens muscles and should be avoided.[10]

An articulated molded ankle-foot orthosis (MAFO); this cosmetic appliance fits into a regular shoe. It allows free dorsiflexion but prevents plantarflexion and hence, toe walking. Photo F.A. Davis 2007 fadavis.com
For toe walking due to muscle spasticity, stretching alone is ineffective.[31] Serial casting can be used to lengthen the Achilles tendon, but the contracture recurs rapidly unless the patient is maintained in an AFO. An articulated molded AFO, if used consistently, is an effective appliance for preventing the progression of spastic equinus that occurs with growth. If a patient with spasticity continues to toe-walk when AFOs are discontinued after the patient reaches skeletal maturity, operative lengthening may then be considered so that the orthosis can be discontinued. After skeletal maturity, equinus in a patient who is spastic is less likely to recur.[9]
Chemodenervation of the gastrocnemius-soleus complex muscles with botulinum toxin is yet another method of nonoperative treatment. Botulinum toxin causes temporary (~3 months) selective muscle paralysis by blocking acetylcholine release at the neuromuscular junction. It was first introduced in the early 1990s as an injection into the gastrocnemius muscle in an attempt to decrease tone in patients with cerebral palsy (CP).[46] Subsequently, its suggested indications expanded to ITW, but most studies have found it to have little efficacy in this application.[34]
A 2014 review of the literature by van Kuijk et al found preliminary evidence for beneficial effects of serial casting and surgery on passive ankle dorsiflexion, as well as on walking kinetics and kinematics, though normalization does not seem to occur.[47] In this article, botulinum toxin type A was not found to improve the results of casting. Only after surgery were sustainable effects lasting longer than 1 year reported. Effectiveness with respect to functional activities and social participation has yet to be demonstrated.
For toe walking associated with paralytic muscle disease, the use of regular stretching and orthoses together should be considered while the child remains ambulatory. Both modalities of nonoperative treatment are preferable to operative lengthening, which weakens the muscle and interferes with ambulation. Prolonged use of serial casts also weakens muscles and should be avoided.[10]
| Surgical Therapy |
If conservative measures fail to correct ITW after about 12 months, operative lengthening can be considered if the ankle equinus is considered to be having a significant impact on the patient’s gait. Complete Achilles lengthening is most commonly performed for ITW and is indicated if ankle equinus exists both with the knee flexed and with it extended. The procedure can be performed under a brief anesthetic by means of either open or percutaneous technique.[8, 29]
An open heel-cord lengthening is performed through either a longitudinal incision approximately 6-8 cm long placed medial to the Achilles tendon or a transverse incision at the level of the malleoli. A longitudinal incision centered over the tendon is avoided in order to decrease the risk of wound dehiscence and because the skin scar may contract and limit dorsiflexion.
The tendon sheath is opened, and the tendon is incised longitudinally over the full length of the exposure, so that it is divided into two equal halves. One half is detached proximally and the other half distally in a Z fashion. The two halves of the tendon are then sutured back together at the desired length. After the procedure, the patient is immobilized in a below-the-knee cast for approximately 6 weeks.
Percutaneous rather than open lengthening of the Achilles tendon is also an option for most patients with ITW. In this technique, an assistant holds the patient’s foot and ankle in maximum dorsiflexion after the skin is prepared. A thin-bladed tenotomy knife is inserted through a small medial stab wound 5-8 cm above the calcaneal insertion, depending on the size of the patient.
By feel, the medial half of the proximal tendon is divided. A second medial stab wound just above the distal insertion is made, and the anterior half of the tendon is divided. If the tendon has rotated a full 90º over this length, half of the fibers have been cut proximally and the other half have been cut distally. The assistant feels the tendon give, and the equinus contracture may then be corrected.
The amount of correction is controlled by immobilizing the foot and ankle in a below-the-knee cast in the desired position. If the tendon fails to part with two incisions, a third stab wound is made from a straight posterior approach, halfway between the first two incisions. Through this, the lateral half of the fibers is cut until the tendon gives.
Open or percutaneous complete Achilles lengthening can also be used to address toe walking in non-ITW, but lengthening must be judicious and may compromise gait function if global gait mechanics are not considered. For example, is the ankle truly in equinus, or is the patient bearing weight on the forefoot because the knee is flexed? If the latter is true, heel-cord lengthening results in a progressive crouch gait with worsened overall function and should therefore be avoided. Such a patient may benefit from lengthening of the hamstrings and possibly the hip flexors, not the gastrocnemius. However, management of complex spastic gait is beyond the scope of this article.
Selective Achilles or gastrocnemius-soleus complex lengthening is often preferred in patients with muscle spasticity so as to avoid excessive weakening of ankle function. The segment of the gastrocnemius-soleus complex that is affected may be distinguished by means of the Silfverskiöld test (see Anatomy).
For example, a patients with hemiplegic spasticity involving one lower extremity would undergo selective gastrocnemius lengthening if the ankle can be brought passively to neutral with the knee flexed but falls into equinus as the knee is extended. The gastrocnemius aponeurosis can be lengthened just before it joins the aponeurosis of the soleus (Vulpius or Baker) or at the gastrocnemius-to-Achilles muscle-tendon junction (Strayer procedure).[7]
Heel-cord lengthening can be considered in a patient with paralytic muscle disease who walks on the toes, but only if the knee extends fully and the quadriceps has normal or near-normal strength. If the patient is using toe walking to generate an extension moment at the knee as compensation for a weak quadriceps, heel-cord lengthening causes premature loss of ambulation. All patients with Duchenne muscular dystrophy (DMD) during their last few years of ambulation use toe walking to compensate for weak knee extensors. Management of toe walking in such patients should be limited to nonoperative modalities (eg, bracing).
| Postoperative Care |
After a heel cord is surgically lengthened, the patient is typically immobilized in a below-the-knee cast for approximately 4-6 weeks. The position of the ankle is thought to be critical if a percutaneous approach was used; the ankle is placed into more dorsiflexion if more lengthening is desired and less dorsiflexion if less lengthening is desired.
Adequate pain control in the acute postoperative setting is imperative both to promote the child’s comfort and to reduce muscle spasms, which may alter the desired surgical correction. The limb(s) should be elevated for 2-3 days until acute swelling resolves. Weightbearing on the limb is routinely permitted if a percutaneous or open sliding tendon lengthening was performed. For patients who underwent open Z-lengthening, some surgeons prefer to defer weightbearing until tendon healing is sufficient (~6 weeks).
| Complications |
The chief concern after operative heel-cord lengthening for treatment of ITW is recurrence. Although recurrence of ITW after surgery is uncommon, the authors have used molded AFOs for as long as 1 year to manage recurrence before considering repeat operative lengthening. The diagnostic workup should be revisited for any patient with recurrent ITW after surgery as a means of looking for signs of neuromuscular disease or intraspinal pathology that might not have been evident initially.
Recurrence after operative heel-cord lengthening is common in neuromuscular diseases, owing to continued spasticity and extremity growth. The appropriate use of an orthosis and stretching can help prevent this complication.
A feared postoperative complication for patients with toe walking secondary to spasticity or paralytic muscle disease is deterioration of independent ambulation. Such complications are minimized through careful preoperative evaluation and judicious selection, as well as meticulous execution of a heel-cord procedure. If function is adversely impacted by tendon lengthening, the foot and ankle should be supported with an orthosis.
Finally, wound dehiscence, necrosis, and cutaneous nerve injury may occur as complications, but they are relatively rare in this setting.
| Long-Term Monitoring |
Once the cast has been removed, the patient may resume walking on the operated limb. A patient with ITW manifests a plantarflexion weakness out of the cast and runs flatfooted. The gastrocnemius-soleus complex typically regains strength slowly over the subsequent few months, returning to normal within 1 year.[48] The patient is usually followed for 1-2 years after the surgical intervention to ensure that toe walking does not recur.
Immature patients with spasticity or paralytic muscle disease should be monitored closely after heel-cord lengthening. With growth or continued muscle fibrosis, contractures are prone to recurrence. In these patients, stretching, orthotics, or both are typically needed during growth to maintain foot position and prevent recurrence.
Source Medscape
| References |
- Habitual toe-walking: evaluation and approach to treatment. Caselli MA, Rzonca EC, Lue BY. Clin Podiatr Med Surg. 1988 Jul. 5(3):547-59. [Medline]
- The development of mature gait. Sutherland DH, Olshen R, Cooper L, Woo SL. J Bone Joint Surg Am. 1980 Apr. 62(3):336-53. [Medline]
- Early onset toe-walking in toddlers: a cause for concern? Pernet J, Billiaux A, Auvin S, Rakatovao D, Morin L, Presedo A. J Pediatr. 2010 Sep. 157(3):496-8. [Medline]
- Treatment of idiopathic clubfoot: an historical review. Dobbs MB, Morcuende JA, Gurnett CA, Ponseti IV. Iowa Orthop J. 2000. 20:59-64. [Medline] [Full Text]
- Functional anatomy of the Achilles tendon. Doral MN, Alam M, Bozkurt M, Turhan E, Atay OA, Dönmez G, et al. Knee Surg Sports Traumatol Arthrosc. 2010 May. 18(5):638-43. [Medline]
- Is idiopathic toe walking really idiopathic? The motor skills and sensory processing abilities associated with idiopathic toe walking gait. Williams CM, Tinley P, Curtin M, Wakefield S, Nielsen S. J Child Neurol. 2014 Jan. 29(1):71-8. [Medline]
- Idiopathic toe walking. Oetgen ME, Peden S. J Am Acad Orthop Surg. 2012 May. 20(5):292-300. [Medline]
- Congenital short tendo calcaneus. Hall JE, Salter RB, Bhalla SK. J Bone Joint Surg Br. 1967 Nov. 49(4):695-7. [Medline]
- The orthopaedic management of the ankle, foot, and knee in patients with cerebral palsy. Green NE. Instr Course Lect. 1987. 36:253-65. [Medline]
- The management of equinus deformity in Duchenne muscular dystrophy. Williams EA, Read L, Ellis A, Morris P, Galasko CS. J Bone Joint Surg Br. 1984 Aug. 66(4):546-50. [Medline]
- McAbee GN. Acute toe walking with viral myositis. Pediatr Neurol. 2013 Nov. 49(5):e11. [Medline]
- Idiopathic toe-walking in children, adolescents and young adults: a matter of local or generalised stiffness? Engelbert R, Gorter JW, Uiterwaal C, van de Putte E, Helders P. BMC Musculoskelet Disord. 2011 Mar 21. 12:61. [Medline] [Full Text]
- The prevalence and course of idiopathic toe-walking in 5-year-old children. Engström P, Tedroff K. Pediatrics. 2012 Aug. 130(2):279-84. [Medline]
- Toe walking: causes, epidemiology, assessment, and treatment. Ruzbarsky JJ, Scher D, Dodwell E. Curr Opin Pediatr. 2016 Feb. 28 (1):40-6. [Medline]
- Persistent toe walking in autism. Barrow WJ, Jaworski M, Accardo PJ. J Child Neurol. 2011 May. 26(5):619-21. [Medline]
- Neuropsychiatric symptoms and problems among children with idiopathic toe-walking. P, Van’t Hooft I, Tedroff K. J Pediatr Orthop. 2012 Dec. 32(8):848-52. [Medline]
- A Comparison of the Birth Characteristics of Idiopathic Toe Walking and Toe Walking Gait Due to Medical Reasons. Baber S, Michalitsis J, Fahey M, Rawicki B, Haines T, Williams C. J Pediatr. 2016 Apr. 171:290-3. [Medline]
- An update on the prevalence of cerebral palsy: a systematic review and meta-analysis. Oskoui M, Coutinho F, Dykeman J, Jetté N, Pringsheim T. Dev Med Child Neurol. 2013 Jun. 55(6):509-19. [Medline]
- Update on the treatment of Duchenne muscular dystrophy. Rodino-Klapac LR, Mendell JR, Sahenk Z. Curr Neurol Neurosci Rep. 2013 Mar. 13(3):332. [Medline]
- Effect of persistent toe walking on ankle equinus. Analysis of 60 idiopathic toe walkers, Sobel E, Caselli MA, Velez Z. J Am Podiatr Med Assoc. 1997 Jan. 87(1):17-22. [Medline]
- Neptune RR, Burnfield JM, Mulroy SJ. The neuromuscular demands of toe walking: a forward dynamics simulation analysis, J Biomech. 2007. 40(6):1293-300. [Medline]
- Muscle compensatory mechanisms during able-bodied toe walking. Sasaki K, Neptune RR, Burnfield JM, Mulroy SJ. Gait Posture. 2008 Apr. 27(3):440-6. [Medline]
- Idiopathic toe walking: a kinematic and kinetic profile. Westberry DE, Davids JR, Davis RB, de Morais Filho MC. J Pediatr Orthop. 2008 Apr-May. 28(3):352-8. [Medline]
- Idiopathic toe walking and contractures of the triceps surae. Solan MC, Kohls-Gatzoulis J, Stephens MM. Foot Ankle Clin. 2010 Jun. 15(2):297-307. [Medline]
- Idiopathic toe-walking: does treatment alter the natural history? Eastwood DM, Menelaus MB, Dickens DR, Broughton NS, Cole WG. J Pediatr Orthop B. 2000 Jan. 9(1):47-9. [Medline]
- The natural history of idiopathic toe-walking: a long-term follow-up of fourteen conservatively treated children. Hirsch G, Wagner B. Acta Paediatr. 2004 Feb. 93(2):196-9. [Medline]
- Serial casting in the treatment of idiopathic toe-walkers and review of the literature. Fox A, Deakin S, Pettigrew G, Paton R. Acta Orthop Belg. 2006 Dec. 72(6):722-30. [Medline]
- Idiopathic toe walking: a comparison of treatment methods. Stricker SJ, Angulo JC. J Pediatr Orthop. 1998 May-Jun. 18(3):289-93. [Medline]
- Comprehensive outcomes of surgically treated idiopathic toe walkers. McMulkin ML, Baird GO, Caskey PM, Ferguson RL. J Pediatr Orthop. 2006 Sep-Oct. 26(5):606-11. [Medline]
- Recurrence after Achilles tendon lengthening in cerebral palsy. Rattey TE, Leahey L, Hyndman J, Brown DC, Gross M. J Pediatr Orthop. 1993 Mar-Apr. 13(2):184-7. [Medline]
- Outcome of 23h Bracing for Tip-toe-walking Children with Cerebral Palsy. Kranzl A, Grasl C, Csepan R, Grill F. Biomed Tech (Berl). 2013 Aug;58 Suppl 1. pii: /j/bmte.2013.58.issue-s1-D/bmt-2013-4120/bmt-2013-4120.xml. doi: 10.1515/bmt-2013-4120. Epub 2013 Sep 7. [PubMed] [PDF]
- Chronologic outcome of surgical tendoachilles lengthening and natural history of gastroc-soleus contracture in cerebral palsy. A two-part study. Damron TA, Greenwald TA, Breed AL. Clin Orthop Relat Res. 1994 Apr. (301):249-55. [Medline]
- Botulinum toxin A does not improve the results of cast treatment for idiopathic toe-walking: a randomized controlled trial.Botulinum toxin A does not improve the results of cast treatment for idiopathic toe-walking: a randomized controlled trial. Engström P, Bartonek Å, Tedroff K, Orefelt C, Haglund-Åkerlind Y, Gutierrez-Farewik EM. J Bone Joint Surg Am. 2013 Mar 6. 95(5):400-7. [Medline]
- Comparing botulinum toxin A with casting for treatment of dynamic equinus in children with cerebral palsy. Ackman JD, Russman BS, Thomas SS, Buckon CE, Sussman MD, Masso P. Dev Med Child Neurol. 2005 Sep. 47(9):620-7. [Medline]
- Idiopathic Toe Walking: Tests and Family Predisposition. D, Ramírez Llamas J, Pomarino A. Foot Ankle Spec. 2016 Aug. 9 (4):301-6. [Medline]
- Electromyography of idiopathic toe walking. Kalen V, Adler N, Bleck EE. J Pediatr Orthop. 1986 Jan-Feb. 6(1):31-3. [Medline]
- Electromyographic test to differentiate mild diplegic cerebral palsy and idiopathic toe-walking. Policy JF, Torburn L, Rinsky LA, Rose J. J Pediatr Orthop. 2001 Nov-Dec. 21(6):784-9. [Medline]
- Electromyographic differentiation of diplegic cerebral palsy from idiopathic toe walking: involuntary coactivation of the quadriceps and gastrocnemius. Rose J, Martin JG, Torburn L, Rinsky LA, Gamble JG. J Pediatr Orthop. 1999 Sep-Oct. 19(5):677-82. [Medline]
- Differentiation of idiopathic toe-walking and cerebral palsy. Hicks R, Durinick N, Gage JR. J Pediatr Orthop. 1988 Mar-Apr. 8(2):160-3. [Medline]
- The kinematic patterns of toe-walkers. Kelly IP, Jenkinson A, Stephens M, O’Brien T. J Pediatr Orthop. 1997 Jul-Aug. 17(4):478-80. [Medline]
- Idiopathic Toe Walking: A Gait Laboratory Review. O’Sullivan R, O’Brien T. Ir Med J. 2015 Jul-Aug. 108 (7):214-6. [Medline]
- The Toe Walking Tool: a novel method for assessing idiopathic toe walking children. Williams CM, Tinley P, Curtin M. Gait Posture. 2010 Oct. 32(4):508-11. [Medline]
- Feedback system based on plantar pressure for monitoring toe-walking strides in children with cerebral palsy. Pu F, Fan X, Yang Y, Chen W, Li S, Li D. Am J Phys Med Rehabil. 2014 Feb. 93(2):122-9. [Medline]
- Whole-Body Vibration Results in Short-Term Improvement in the Gait of Children With Idiopathic Toe Walking. Williams CM, Michalitsis J, Murphy AT, Rawicki B, Haines TP. J Child Neurol. 2016 Aug. 31 (9):1143-9. [Medline]
- Management of cerebral palsy with botulinum-A toxin: preliminary investigation. Koman LA, Mooney JF 3rd, Smith B, Goodman A, Mulvaney T. J Pediatr Orthop. 1993 Jul-Aug. 13(4):489-95. [Medline]
- Treatment for idiopathic toe walking: a systematic review of the literature. Kuijk AA, Kosters R, Vugts M, Geurts AC. J Rehabil Med. 2014 Nov. 46 (10):945-57. [Medline]
- Outcome of patients after Achilles tendon lengthening for treatment of idiopathic toe walking. Hemo Y, Macdessi SJ, Pierce RA, Aiona MD, Sussman MD. J Pediatr Orthop. 2006 May-Jun. 26(3):336-40. [Medline]